History
of Modern Gynecology
Many people are unaware of how
modern gynecology was started and how men (doctors and male-midwives)
took over providing gynecological procedures and childbirth
when medical school was invented. Before modern medicine, men
were not allowed to be present at births or other procedures
that dealt with the intimate parts of women.
Many midwives when medical schools were established bitterly
opposed the involvement of men in childbirth. Some male practitioners
also opposed the involvement of medical men like themselves
in midwifery and even went as far as to say that male-midwives
only undertook midwifery solely for perverse erotic satisfaction.
Midwives played a role in the
development of obstetrics. For through most of the twentieth
century, midwives have been thrust to the sidelines. Fortunately,
midwifery is making a comeback and thousands of women enjoy
the care of midwives and OBs. Either way, midwives are the ones
who have assisted women during labor for thousands upon thousands
of years. Without them, and their copious amount of knowledge,
the first rung of obstetrics would never have been climbed.
In fact, until the 20th century, the science of Obstetrics was
still referred to as Midwifery in medical schools – and
obstetrix is the Latin word for midwife!
Once the field of medicine and the arena of pregnancy and childbirth
were usurped by modern medicine – all doctors, including
obstetricians were men. The first female to graduate from medical
school was Elizabeth
Blackwell back in 1849, although it took more than a century
and a half for female doctors to be considered “normal.”
Some Historical Facts About How Male
Gynecologists Evolved:
1) Dr. James Marion Sims
from South Carolina is said to have invented modern gynecology
in America. He is considered the “father of modern gynecology”.
Dr. Sims is known for inventing gynecological techniques we
still use today; most notably he invented a surgical technique
to repair vesicovaginal fistula. Beginning in 1845 Dr. Sims
developed a surgical technique to cure this taboo medical condition
through experimentation on human subjects. What makes Dr. Sims’
experimental techniques so horrific is that he used enslaved
black women as human subjects for his research and because these
women were considered to be property, they could not consent
to these appalling procedures. In fact, their owners were allowed
to consent for them, owners with a strong financial interest
in the success of these surgeries. Even worse, Dr. Sims performed
these surgical procedures on black women without anesthesia
because of his belief that black women were not capable of feeling
pain; however, the very real pain of Betsey, Anarcha, and Lucy
are detailed in Dr. Sims’ many journals. Not only did
Dr. Sims violate these women without their consent, he also
invited people to watch as he performed these experimental surgeries,
further stealing the dignity of the women who were forced to
partake in his research. Dr. Sims performed 35 surgeries on
one single human subject, Anarcha, before completing a single
“successful” surgery.
2) In October 1889, Dr. Howard Atwood
Kelly was appointed the first professor of gynecology
and obstetrics, and is universally regarded as establishing
gynecology as a surgical specialty.
3) By the late 19th century the foundation of
modern day obstetrics and midwifery began develop. Delivery
of babies by doctors became popular and readily accepted, but
midwives continued to play a role in childbirth.
4) The American College of Obstetricians
and Gynecologists (ACOG) founded in 1951 is a professional
association of physicians specializing in obstetrics and gynecology
in the United States. It is an organization with a membership
of approximately 58,000 obstetrician-gynecologists and women's
health care professionals. A majority of ob/gyns in 1951 were
males.
Look at this important section about historical
progression of pelvic exams in the article, Male
physicians treating Female patients: Issues, Controversies and
Gynecology below:
“The oldest medical text
known to man is the "Kahun Gynecological Papyrus",
written by the Egyptians around 1800 BCE. The papyrus provides
a glance into early gynecological medicine and unveils the traditions
of reproduction, conception and delivery in ancient Egypt. For
the Egyptians, the main treatment modalities provided by the
"swnw" (pronounced sounou, physician figure) were
founded on pharmacopoeia from animals, plants and minerals;
surgical intervention was never recommended (2). Magic spells
were whispered, as it was believed that diseases were demonic
in origin.
Due to compliance with
religious doctrine, men were not allowed to be present at births
or at other rituals that dealt with the intimate parts of a
woman. Instead, it was the role of the midwife to take
care of women and to assist them with their gynecological needs.
Interestingly enough, the "Kahun Papyrus" provides
some of the earliest evidence of midwifery in history.
Similarly, in the middle ages,
it was often the norm for a woman's sexual organs to be examined
by midwives, nurses or other females who previously had had
similar problems to the patient's. By the early 1800's,
with the advent of modern medical degrees and physical examinations,
the pelvic exam began to be performed by male physicians, as
women were not allowed to enroll in medical school.
However, this examination was a variation of the modern version
as it consisted of a "compromise" in which the physician
kneeled before the woman but did not directly inspect her genitals,
only palpated them.
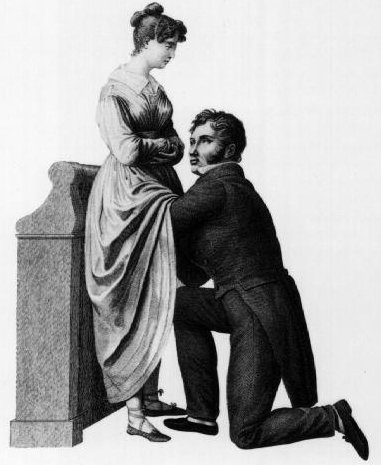
The historic taboo associated
with the examination of female genitalia has long inhibited
the science of gynecology. This 1822 drawing by Jacques-Pierre
Maygrier shows a "compromise" procedure, in which
the physician is kneeling before the woman but cannot see her
genitalia. Modern gynecology no longer uses such a
position. The above picture is when they first introduced men
to do gynecological procedures on women.
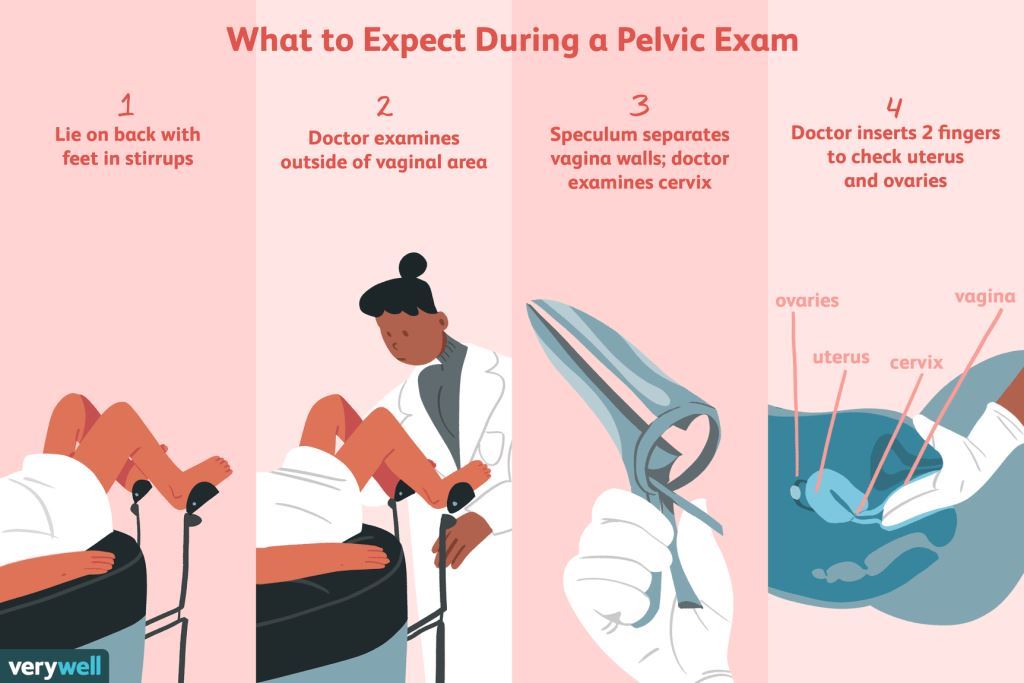
Source:
Illustration by Emily Roberts, Verywell
The above picture is of how a pelvic exam is performed today.
Speculum in 3 above is used for the Pap smear.
In addition, it
was during this period that the use of a chaperone became a
part of the clinical examination. The chaperone's role was to
emotionally support and reassure the patient during a procedure
that she found embarrassing or uncomfortable. The chaperone
also acted as a witness in cases of malfeasance by the physician.
Today, in many parts of the world where religious and cultural
precepts often discourage female encounters with male physicians,
chaperones still attend gynecological examinations.
The truth is chaperones are pretty useless.
They are just there to protect the doctor. Check out the truth
about chaperones by looking at this article, Do
Chaperones Really Protect Patients? and
ACOG's Recommendation
for Chaperones in Preventing Sexual Abuse By Doctors Is Useless.
By the 1970's, only 9% of enrolled
medical students in the United States were women (3). The numbers
have drastically increased since then: now 58% of medical students
are women (4), yet there are still disparities in gender among
the specialties. In Obstetrics and Gynecology, female residency
enrolment rates have quadrupled from 1978 to the present, leaving
men in the minority (women account for 71.8% of Obs/Gyn residents
today). Between 1989 and 2002, the proportion of female Ob/Gyn
residents rose from 44% to 74% while the proportion of female
graduating medical students only increased from 33% to 44% (5).”
Modern medicine has worked to
indoctrinate us that the gender of a gynecologist does not matter.
Male gynecologists often charm women into accepting them due
to their impressive surgical skills & training, compassion,
and gentleness. Many male gynecologists who have sexually abused
women were very professional, compassionate & gentle, and
skilled.
Our culture sees doctors as experts on the body and the medical
industry has worked to indoctrinate even the most modest women
(those with very strict standards such as not wearing a 2 piece
bathing suit and no sex until marriage) to accept that male
gynecologists are okay over the past few centuries since modern
medicine started. Because most gynecologists were males until
recently, women of the past few generations conditioned their
daughters to go to male gynecologists because that’s what
their mothers did. This is a huge cultural blind spot. This
also proves that doctors have so much power in our society.
Think about this scenario:
A teenage daughter
has a tampon stuck and she needs help to retrieve it. Her mom
tried to retrieve it, but could not. The girl's father is better
than her mother at retrieving things. Would it be appropriate
for the girl's father to retrieve the tampon simply because
he is more experienced than his wife? If the girl's mom cannot
retrieve the tampon, they should look for another woman to retrieve
it. The same should be true of doctor. You should look for a
female doctor until you find the one that is skilled for your
case.
The truth is most people in our society would accuse the father
in the above scenario of incest if he helped to remove a tampon
from his teenage daughter even if he had great intentions, but
they would not look down on a male doctor removing the teenage
girl’s tampon simply because he is a doctor. This is ridiculous
because a male doctor is still a man.
If indeed the pelvic exam is a simple medical
procedure, then a male doctor should not hesitate to perform
an intimate exam on his own mother or his own
daughter, or his grandmother,
or any other female relative! Of course the
mere thought of such an intimate exam on a close relative is
alarming and disgusting to consider. Why? Because it raises
the image of incest – sex among relatives, one
of the most forbidding actions in human behavior. From
this simple illustration we know positively that a pelvic exam
is loaded with sexuality – it is not a mere medical procedure.
In denying the sexuality of the pelvic exam for a century, the
medical profession has been committing a fraud – a deliberate
misrepresentation – on female patients. Sons do not look
up their mother’s skirt and fathers do not look up their
daughter’s skirt.
While it is great that modern gynecology has
brought improvements such as C-Sections that have cut down on
maternal deaths, surgeries for gynecologic cancers, etc., only
women should have been allowed to be gynecologists in the beginning.
Medical school made a big mistake by only allowing men to become
gynecologists. Thankfully, there has been a big increase in
female gynecologists in the 21st century. Sexual abuse and voyeurism
by male doctors would have never happened if male doctors were
prohibited from doing intimate procedures on women.
Many women dread having gynecological procedures
(they see no sexual connotations to those procedures) so they
assume that it is impossible for a male doctor to have any lustful
thoughts especially because they do gynecological procedures
all of the time. Also, many women are so focused on making sure
they do not have cancer and this is why they submit to gynecological
procedures. But the truth is men (no matter how good their intentions
are) often have lustful thoughts when they see a woman’s
private parts. Male doctors are no different from other men.
Male doctors often have normal sex lives; many of them are married
with children.
Women and men differ in their sexual responses. Rare is the
man who can approach the idea of being asked to touch a naked
female in her intimate parts in any context without a hint of
sexuality entering his mind. Females are usually only eroticized
by proper mood and situation, but the male sexual response is
visual, tactile and immediate. This is exactly why women rarely
think about how a gynecological procedure could be sexual for
a male doctor.
Sadly, some female gynecologists are very insensitive to women’s
modesty today because they see nothing wrong with referring
a woman to another male doctor such as a gynecologic oncologist
or fertility specialist. Many female gynecologists rotate with
male gynecologists who could deliver their patients’ babies.
Also, some female gynecologists use male medical personnel such
as medical students, residents, nurses, etc. to assist them
with gynecological procedures. Some female gynecologists have
been desensitized in medical school that gender does not matter
and that modesty is not important.
All women are encouraged to read this book,
Women
and Doctors by Dr. John Smith (Dell Publishing,
1992) that exposes the gynecology industry and how women are
often mistreated by male gynecologists. Make sure you especially
read the chapters, 3 – The Behavior of Doctors
in General and 4 – The Miscasting of
Males As Gynecologists. The book is outdated on some
medical procedures such as pap smears and pelvic exams, but
those two chapters are still relevant today in 2018. His chapter
on unnecessary surgeries is still relevant because a lot of
unnecessary hysterectomies are done today.
Dr. John Smith is a former male gynecologist
who courageously shared that after 24 years of medical
education and clinical gynecological experience that men should
not be gynecologists. He shared that he had to do a
lot of soul-searching as a male gynecologist. “Male gynecologists,
like all men, go through the kind of ‘attitude setting’
that occurs in the proverbial locker rooms while they are growing
into manhood.” Dr. Smith, whose practice was in Colorado
Springs, says that “It is common and acceptable among
practicing gynecologists to speak about their patients' bodies,
sexual behavior, or medical problems indiscriminately, in terms
that are demeaning and reflect a lack of kindness and respect.”
(p. 32) Becoming more explicit, he charges them with eroticizing
the medical scene: “It is a rare male who is able to see
women day in and day out, examine their bodies, hear details
of their sex lives, and not only never have a lascivious thought
or abuse that access but always remain clinical…”
(p.34) He confesses that “I have had a colleague invite
me to do an exam on one of his patients under the false guise
of a consultation because ‘she has a body you won’t
believe’.” “I have seen a physician walk out
of an exam room and tell a hallway full of doctors and nurses
about the disease his married patient had contracted as a result
of an affair. I have seen more than one gynecologist walk into
an operating room where another doctor’s patient was already
asleep for surgery, lift up the sheet, admire the patient’s
breasts, and continue his conversation without pause.”
(p.32-33) Dr. Smith concluded dramatically: After twenty-four
years of medical education and clinical gynecological experience,
it is my opinion that males should not be gynecologists. The
role properly belongs to women.” (p.34).
Dr. John Smith also made some other
important points in the book:
1) At this point, many of you are saying “not
my doctor, my doctor is honest, competent, and has only my welfare
at heart. Please understand that a pleasant demeanor and impressive
diplomas and certificates do not mean your doctor is incapable
of the behavior I will describe in this book. (page 3) - This
is true. Many of the male gynecologists who have abused women
fool their patients by their professionalism, knowledge, and
compassion.
2) No other professional in America enjoys
the degree of authority that physicians have managed to secure.
Almost unquestioned in their judgments, they have been given
the authority to exercise power in areas that extend beyond
their medical area of competence. Physicians can also decide
if you should be allowed to do certain kinds of work or if you
can play a sport in school, and can exercise unquestioned power
in myriad other aspects of your life. (page 23). - This
is true. Many of doctors push patients into making decisions
that they would not normally make in another setting.
3) Too often, women rely on the gynecologist’s
“reputation,” and if it appears to be good they
assume the gynecologist, too is good. It is rare to hear information
about how bad a doctor is, except from former patients, and
they often do not have a large audience. It’s much more
common today to hear, in a hospital’s advertisements for
instance, that their staff physicians are all terrific, well-trained,
caring, and attentive (page 117). – This is very
true. In fact, many doctors are able to have their negative
reviews from patients on web sites removed. One hospital in
Ohio continued to show an ad about how wonderful one colorectal
surgeon was even after he had anally raped a patient.
4) What do you call it if a doctor subjects
your daughter to a breast and pelvic exam when there is no medical
indication for it and your daughter did not ask for it? Is it
any less a sexual assault than her being fondled and disrobed
by a date who thinks he “has the right’? (page 37)
– This is very true.
5) In recent years, we have recognized the
seduction of a woman by her psychiatrist, is in fact, a criminal
act. Similar abuse occurs in the gynecological setting, but
it is called something else. Perhaps because women have not
felt sufficiently empowered to threaten gynecologists’
positions, these doctors have not been subjected to the same
level of scrutiny as other professionals (page 37). –
This is very true. So many gynecologists can get away
with abusing women. Many women are too embarrassed or scared
to report their gynecologists. Many women want to report their
doctors anonymously, but this is not possible so they just stay
silent. Also, most medical boards won’t do much about
gynecologists who have abused women.
6) Hysterectomies are deliberately
sold to women by doctors who use the operation as their major
source of income. They are done by well-meaning but misguided
physicians who believe women are better off without their uterus.
Mostly they are done by male physicians who were trained in
a milieu that did nothing to alter their ingrained male prejudices
about women and that reinforced the attitude that it is all
right to decide for a woman what she needs, instead of giving
her knowledge and power to make the decision for herself (pages
47-48).
This is true. The United States
has the highest rate of hysterectomy in world. Approximately
600,000 hysterectomies performed each year in the United States.
It is estimated that 85% to 90% of all hysterectomies are unnecessary
so it is important for women to get a second opinion preferably
from a naturopathic or integrative medicine physician and do
some research on alternative options before they proceed with
a hysterectomy. Gynecologists, hospitals and pharmaceutical
companies make more than $17 Billion dollars a year from hysterectomies.
Also, male gynecologists are more likely to do unnecessary hysterectomies
on women. In fact, one ob/gyn practice in North Carolina that
has 3 male gynecologists has a very high hysterectomy rate.
They’ve done so many unnecessary hysterectomies on women
mostly for benign conditions including one on a lady in her
70s for a prolapsed bladder that was unnecessary.
Some doctors use scare tactics to push women into having a hysterectomy
such as telling her that she could develop cancer later due
to endometriosis or another benign condition that she has. Also,
many doctors tell post-menopausal women and women who do not
plan on having any more children that hysterectomy is a good
option for them without telling them the long term risks such
as heart disease, high blood pressure, etc. they could develop
as a result of the hysterectomy later in life.
Hysterectomy is only medically necessary for saving
a woman’s life. Hysterectomy should only be done in the
case of several life-threatening conditions:
• Invasive cancer of the uterus, cervix, vagina, fallopian
tubes, and/or ovaries
• Unmanageable infection such as gangrene
on uterus that could cause sepsis
• Unmanageable bleeding
• Serious complications during childbirth,
such as a rupture of the uterus
We encourage all women to take time to read
the article, Why
Are Hysterectomies Often Unnecessary? Especially read the
article, Hysterectomy
may have long-term health risks by a female gynecologist
at Mayo Clinic under Sources. It is very interesting that a
male gynecologist in that article argued that women should not
cancel hysterectomy due to possible long-term health risks.
We also encourage all women to take time to
read the articles, Are
Pap smears Necessary for Virgins?, Truth
about Pap Smears, and Truth
About Pelvic Exams.
ACOG has misguided guidelines about pap smears and pelvic exams
because they have the same guidelines for all women and age
groups. The truth is pelvic exams are basically useless for
healthy women who are not pregnant with no symptoms. ACOG does
not address that some women may be at a higher risk for cervical
cancer while some women such as complete virgins who have never
engaged in any kind of sexual activity basically have O% risk
for cervical cancer. 99% of cervical cancer cases are caused
by HPV, a Sexually Transmitted Disease. Pap smear is a screening
test for cervical cancer only. Ovarian cancer is extremely rare
and the most reliable way to diagnose ovarian cancer is through
an ultrasound or blood test — not a pelvic exam.
** We are distributing
stapled 12-page
booklets to women about how they can protect themselves
in medical settings and we are seeking volunteeers to help with
distributing those booklets. We also need some financial support
to pay for more booklets. You
can see what the front cover of the booklet looks like by downloading
this link.
You can purchase booklets from this link.
If you would like to volunteer to distribute booklets or support
us financially, please
Sources:
Do
Chaperones Really Protect Patients?
Male
OB/Gyns in the News
Gentlemen
Don’t Look Up Ladies’ Skirts
Women
and Doctors By Dr. John Smith
Obstetrics
Gynaecology
Let’s
Honor the Mothers of Modern Gynecology
What
Is a Pelvic Exam?
|
